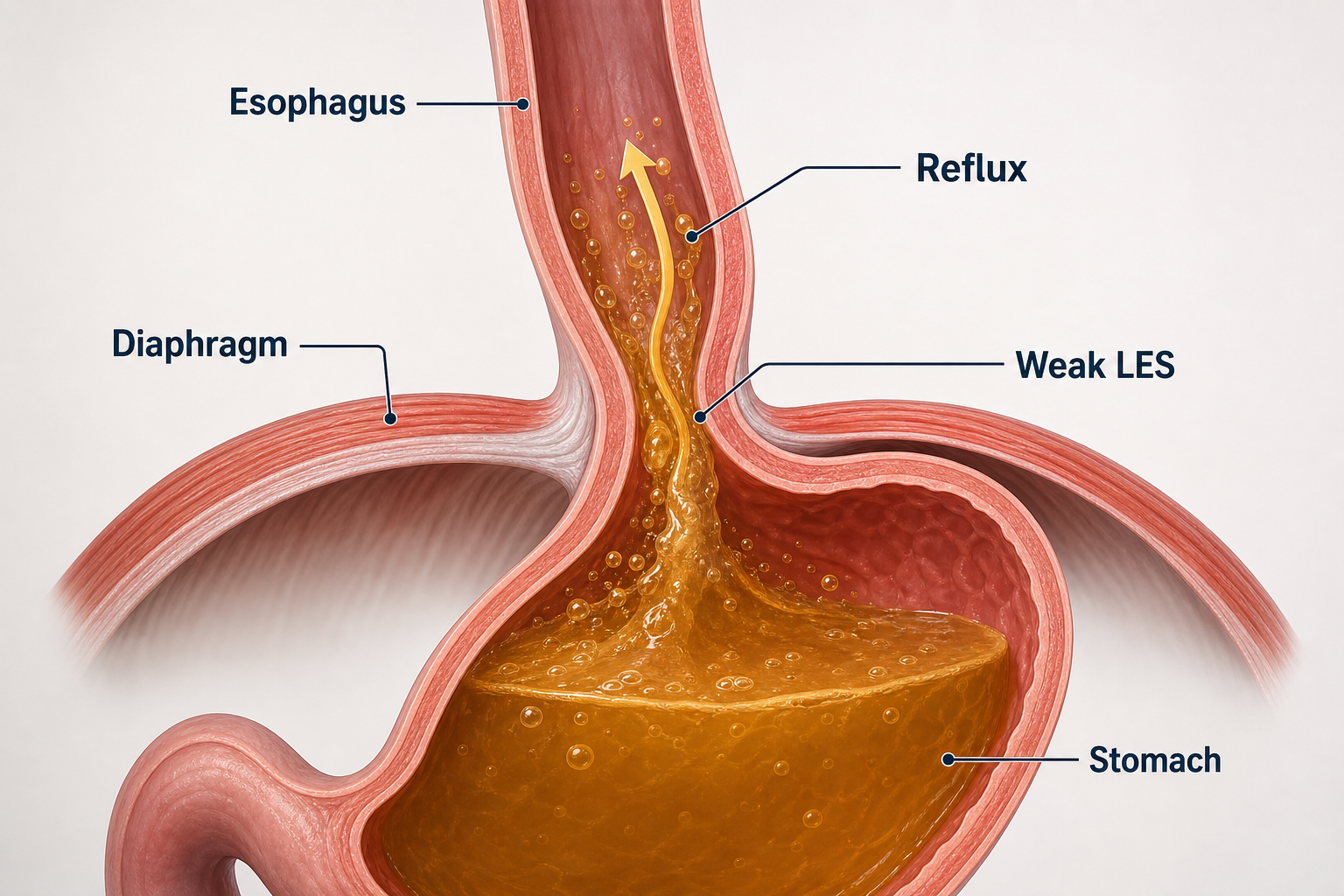
Reflux is a barrier failure
The lower esophageal sphincter, called the LES in US spelling and often LOS outside the US, should keep stomach contents down.
GERD in the US. GORD in the UK, Australia and much of the world.
A practical guide to heartburn, regurgitation, cough, aspiration risk, upper endoscopy, pH testing, medicines, lifestyle measures, Nissen fundoplication, partial wraps, LINX, TIF, redo surgery and reflux after bariatric surgery.
The lower esophageal sphincter, called the LES in US spelling and often LOS outside the US, should keep stomach contents down.
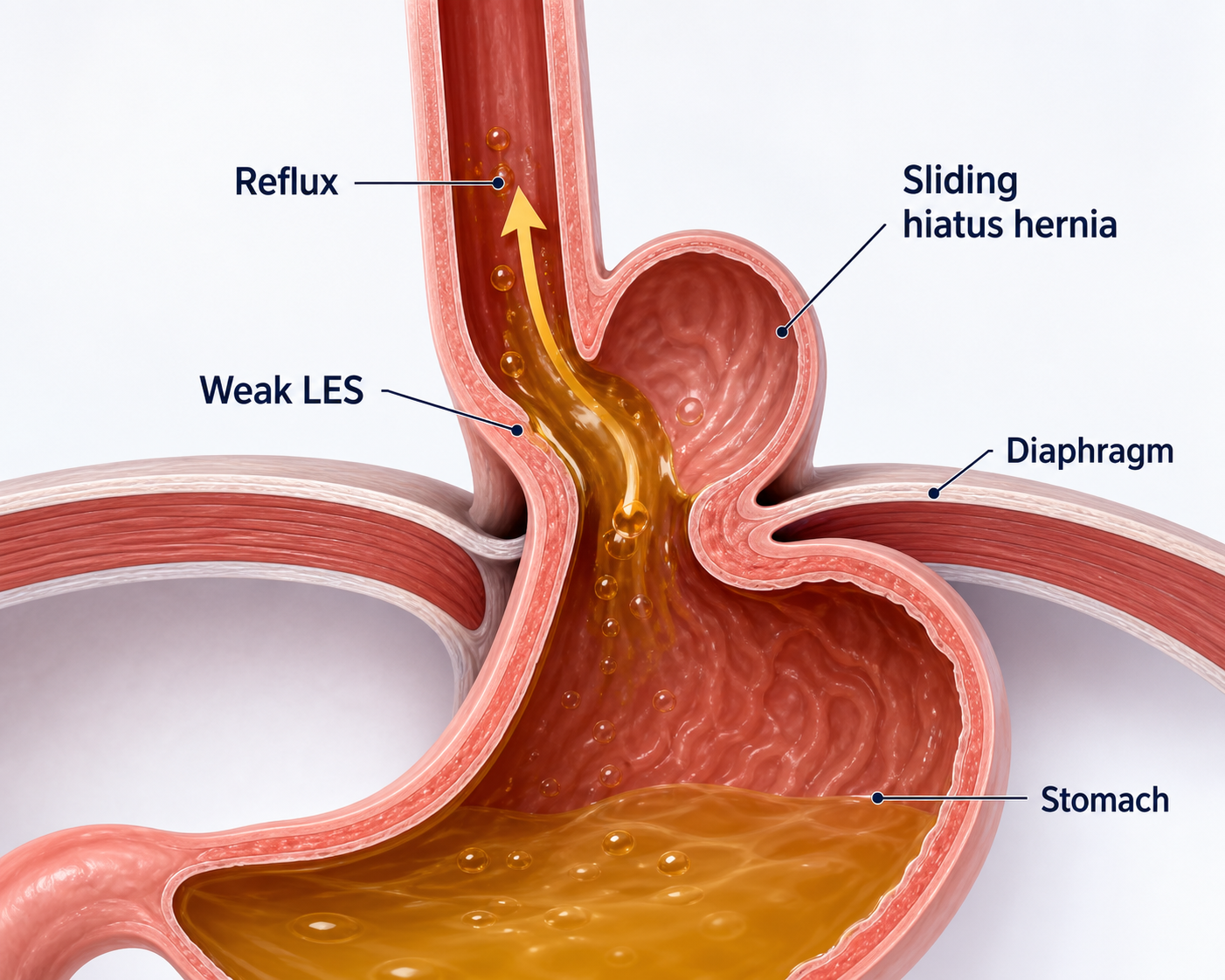
A sliding hiatus hernia moves the valve area above the diaphragm. Some people have weak LES/LOS, hernia, or both.
Upper endoscopy checks esophagitis, strictures, cancer signals, and Barrett's esophagus. pH testing proves reflux burden when needed.
For selected patients with proven reflux, fundoplication can be life-changing, especially when regurgitation or medication dependence dominates.
Anatomy first
The esophagus passes through the diaphragm into the stomach. At that junction, the lower esophageal sphincter (LES; lower oesophageal sphincter or LOS outside the US) and the diaphragm normally work together as an anti-reflux barrier.
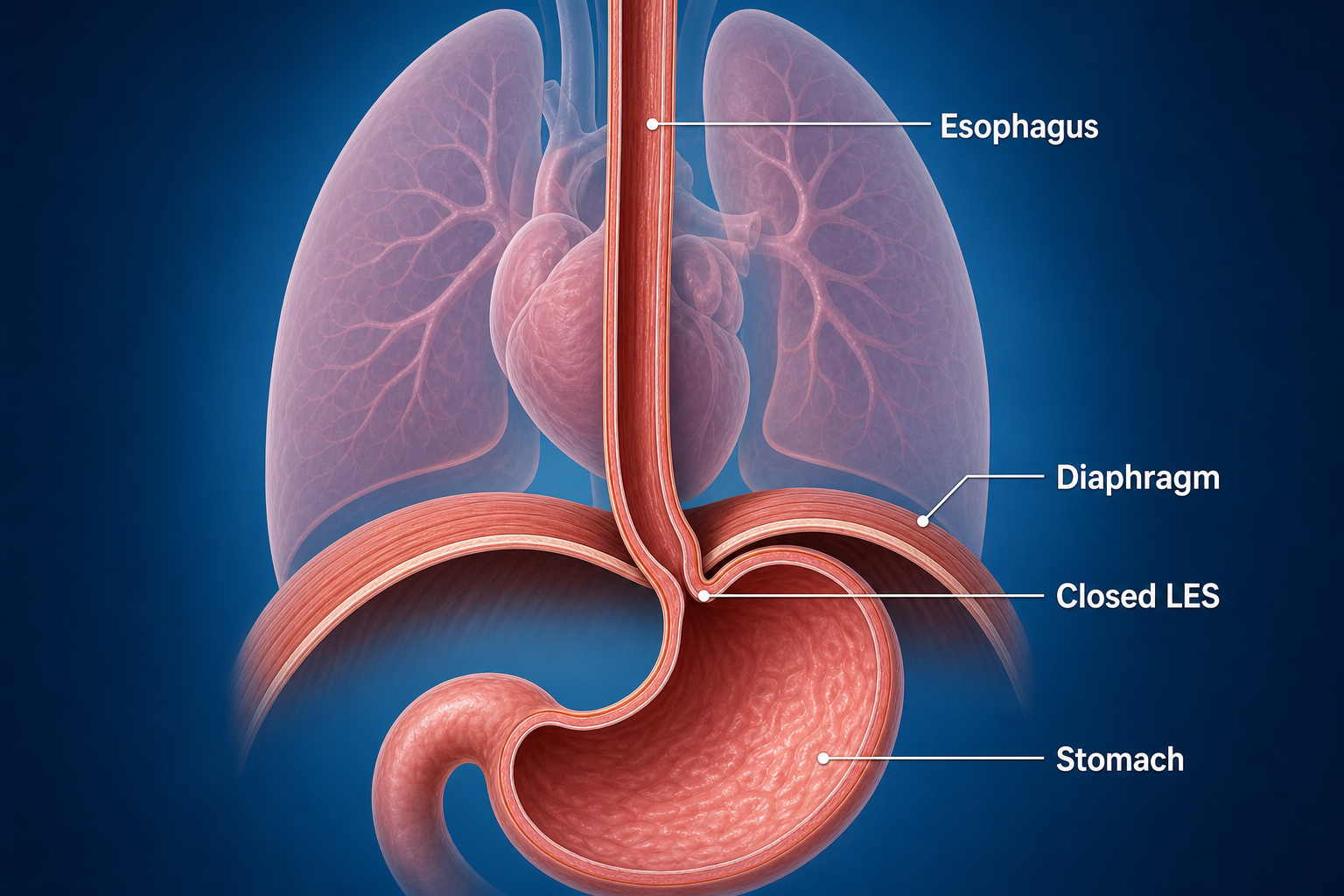
Fasting stomach acid is often around pH 1 to 3. That is normal in the stomach, but not normal bathing the esophagus, throat or lungs. Reflux is not only "acid": it can include pepsin, bile, food, gas, weakly acidic fluid, or non-acid volume reflux, which is why some people still cough or regurgitate on PPIs.
Hiatus hernia
A hiatus hernia means part of the stomach has moved through the diaphragm opening where the esophagus passes. It can exist with reflux, without reflux, or be one piece of a bigger reflux problem.
The common type. The stomach-top and gastroesophageal junction slide upward, weakening the diaphragm-sphincter partnership and often worsening regurgitation.
Less common but more structurally important. Part of the stomach sits beside the esophagus; larger ones can cause anemia, chest pressure, obstruction or volvulus risk.
Sliding plus paraesophageal features. Surgeons usually think about size, symptoms, anatomy, age, frailty and operative risk.
You can still have severe reflux with normal-looking diaphragm anatomy if the sphincter relaxes too often or has low pressure.
Symptoms and complications
Reflux pain is often central, behind the breastbone or lower chest, and may rise toward the throat. It can be worse after meals, bending, lying flat or waking from sleep. New, severe, exertional, crushing or left-arm/jaw-associated chest pain still needs heart causes considered first.
Reflux pain is sometimes misdiagnosed when the problem is actually cardiac. Even if you already have GERD or GORD, call emergency services if chest pain is worse than usual, different, not relieved like normal with antacids, associated with breathlessness, sweating, faintness, jaw/arm/back pain, or just feels wrong.
Ask your gastroenterologist, endoscopist or surgeon before sedation or anesthesia whether the story could be cardiac, especially in older patients or anyone with diabetes, smoking history, high blood pressure, high cholesterol, family history or exertional symptoms. A normal ECG alone does not exclude coronary artery disease; sometimes a stress test, CT coronary angiogram or cardiology review is the more relevant question.
Night-time coughing, waking choking, hoarse voice, throat clearing, sour taste, dental erosion, asthma-like symptoms, recurrent bronchitis or pneumonia can be reflux-related. Silent aspiration can injure lungs over time, especially when regurgitated fluid reaches the airway during sleep.
Extra-esophageal reflux is trickier to prove than classic heartburn. ENT, respiratory and allergy causes may need to be ruled in or out before surgery is blamed or promised.
Diagnosis
Main test for esophagitis, strictures, ulcers, cancer signals, hiatus hernia clues and Barrett's. Biopsies confirm Barrett's and dysplasia.
Measures acid exposure and symptom association. Impedance can detect weakly acidic or non-acid reflux. Often important before surgery.
Checks esophageal muscle function and LES/LOS location. It helps avoid wrapping a poorly moving esophagus too tightly.
Still useful for anatomy, hernia size, obstruction, shortened esophagus, strictures, motility clues and prior surgery. Not a stand-alone GERD test.
Inflammation to Barrett's
Reflux can inflame the esophagus. Endoscopists often grade erosive esophagitis using the Los Angeles system: A and B are milder breaks; C and D are more extensive. Barrett's esophagus means the lining has changed toward an intestinal type, confirmed on biopsy, and needs long-term specialist follow-up.
Often heals on adequate acid suppression. Symptoms do not perfectly predict damage, so endoscopy matters when risk factors or red flags are present.
Higher relapse risk and stronger evidence of true reflux disease. Long-term PPI or anti-reflux surgery discussions become more concrete.
Nondysplastic Barrett's usually means surveillance endoscopy every few years; dysplasia may need expert pathology review and endoscopic eradication therapy.
Do not normalize years of severe reflux, nocturnal regurgitation or swallowing trouble. Early diagnosis, weight reduction when relevant, correct medication use, and timely surgical assessment for mechanical reflux may prevent strictures, long-term inflammation and late discovery of Barrett's.
Non-medical measures
These measures are not a moral test. They are experiments to reduce pressure, volume and night-time exposure.
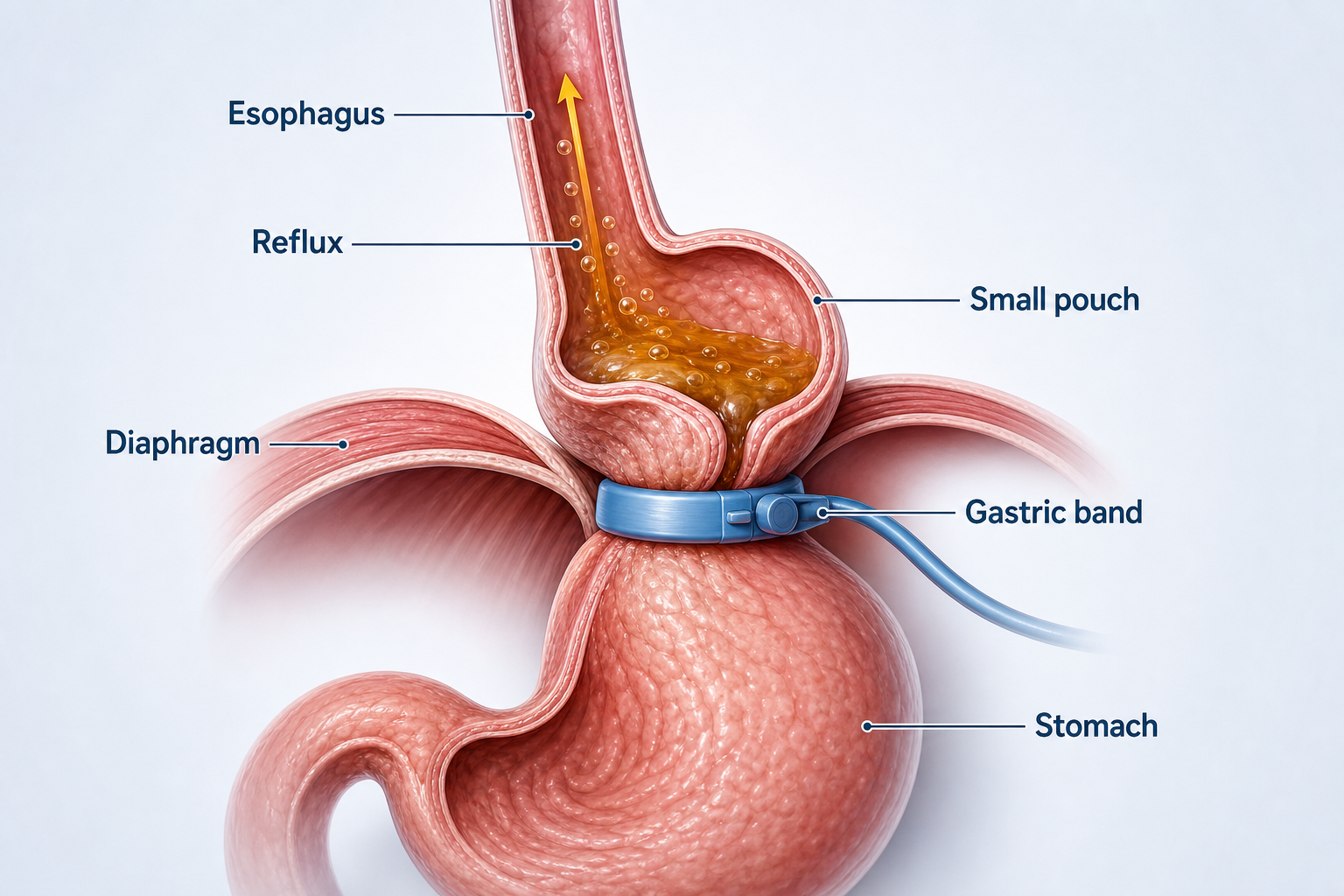
Abdominal pressure drives reflux. Even modest weight loss can reduce symptoms; major weight loss can transform reflux risk for some people.
A wedge or raising the bedhead 6-10 inches helps gravity. Extra pillows often bend the waist and may not help much.
Avoid large late meals. Many people do better not eating within 2-3 hours of lying down.
Trial alcohol reduction, smaller meals, less fat, less chocolate/peppermint/coffee, and avoiding foods that repeatedly trigger your reflux.
Medicines
Omeprazole, esomeprazole, pantoprazole, rabeprazole and lansoprazole block the proton pump in stomach acid-producing cells. They work best taken before meals and are the strongest acid suppressors.
Famotidine reduces acid signaling through histamine-2 receptors. It can help milder reflux, breakthrough night symptoms or step-down therapy, though tolerance can develop.
Tums, Quick-Eze, Rennie and many chewables are usually carbonates such as calcium or magnesium carbonate. Some products use sodium bicarbonate, hydroxides or alginates.
Alginates can react with stomach acid to form a floating "raft" near the top of the stomach after meals. It really can help some post-meal regurgitation, but it does not repair a hiatus hernia or weak LES/LOS.
Milk may briefly buffer acid, but fat/protein can later stimulate more acid and fullness. It is not reliable treatment for frequent GERD/GORD.
Observational studies link PPIs with kidney disease, fractures, infections, low magnesium, B12/iron issues, pneumonia and dementia signals, but association is not proof of causation. The practical question is whether you still need the dose, whether the diagnosis is proven, and whether mechanical reflux would be better treated mechanically.
Anti-reflux surgery
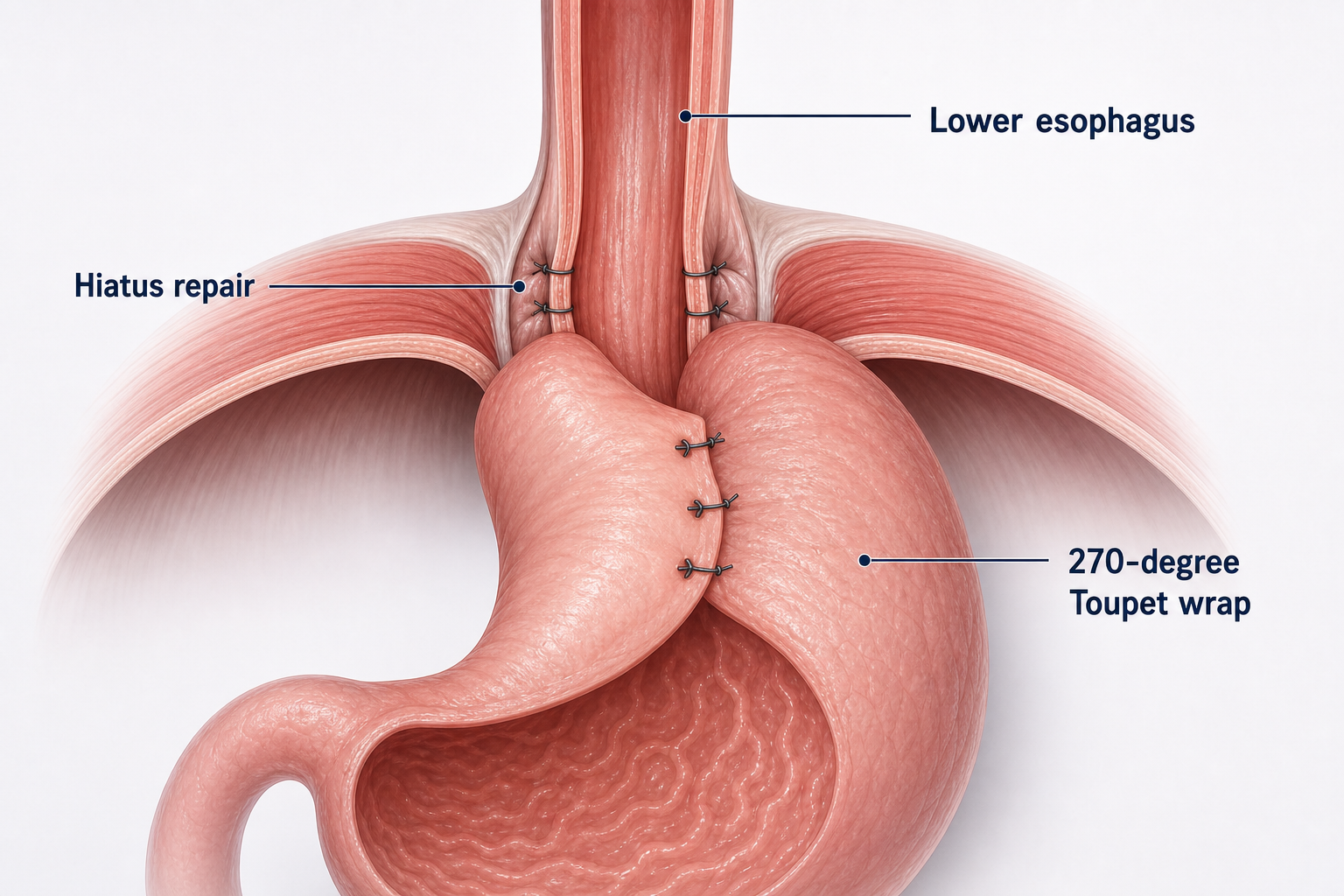
Laparoscopic anti-reflux surgery usually repairs the hiatus hernia if present, brings the stomach back below the diaphragm, narrows the hiatus, and wraps the upper stomach around the lower esophagus to reinforce the LES/LOS.
Names such as Nissen, Toupet, Dor, Thal and Nissen-Rossetti are useful shorthand, but most patients do not need to memorize them. The practical questions are whether reflux is proven, whether a hiatus hernia needs repair, whether manometry shows safe swallowing function, how tight the wrap should be, and how often that surgeon sees dysphagia, dilation, redo surgery or recurrent reflux.
Most operations use keyhole ports under general anesthesia. The surgeon frees the upper stomach and lower esophagus, reduces any hiatus hernia, closes the enlarged hiatus with sutures, then forms a wrap around the lower esophagus. A straightforward case with a proficient team may take about one to two hours; complex redo or giant hernia surgery can take much longer.
When the diagnosis and anatomy are right, reflux relief can be immediate. Swallowing is deliberately respected early because swelling around the new wrap is normal.
Recovery and eating after surgery
Protocols vary by surgeon. This is a typical pattern for uncomplicated laparoscopic fundoplication or hiatus hernia repair, not a substitute for the discharge plan.
Hospital discharge the same day or after one night is common. Sip fluids, walk, use simple analgesia, and expect bloating or shoulder-tip pain from laparoscopy gas/diaphragm irritation.
Liquids to purees or very soft foods, depending on the surgeon. Small frequent meals, chew obsessively, no gulping, no fizzy drinks if they bloat you.
Soft diet expands gradually: eggs, fish, pasta, mince, soups, soft vegetables. Avoid steak, crusty bread, dry chicken and large tablets until swallowing is clearly easy.
Many people return toward normal eating. Desk work may be 1-2 weeks; manual lifting can need 4-6+ weeks. Redo or giant hernia repairs can be slower.
Many patients describe the pain as broadly comparable to other laparoscopic upper-abdominal operations such as gallbladder or bariatric surgery, though individual pain varies. Shoulder-tip pain is common after laparoscopy because gas or a little blood/fluid can irritate the diaphragm; it may last hours to a few days.
Consent reality
Dysphagia can occur early from swelling or a tight wrap. Some patients need dilation; rarely redo surgery or wrap takedown is needed.
Burping or vomiting may become difficult. Bloating, early satiety, flatulence and inability to vent gas can be frustrating.
Bleeding, infection, perforation, pneumothorax, anesthesia complications, vagal nerve injury, delayed gastric emptying and persistent pain are uncommon but real.
Early dumping can cause diarrhea, cramping, flushing or palpitations within about an hour. Late dumping can cause reactive hypoglycemia 1-3 hours after eating.
Functional heartburn, rumination, achalasia, eosinophilic esophagitis, gastroparesis or cardiac disease can masquerade as reflux. Testing matters.
Severe lifelong reflux can mean strictures, Barrett's surveillance, sleep disruption, aspiration, chronic cough and lifelong high-dose medication.
Anti-reflux surgery is usually done under general anesthesia. Reflux itself, obesity, sleep apnea, delayed gastric emptying, GLP-1 medicines, diabetes, lung disease, previous aspiration and redo surgery can all change the anesthesia plan. For a separate patient guide, see AnesthesiaRisks.com.
Weight-loss surgery and reflux
A lived-experience page
The author had severe reflux from childhood, Barrett's by age 18, a fundoplication that failed after about a year, 15 years of double-dose PPI, then a redo by an experienced surgeon that has worked for a decade. The dumping-syndrome story took an unusual turn.
Read the personal storyProvider finder
Choose a category and enter a city, postcode, country, "near me", or a place you might travel.
For surgery, look for an upper GI, foregut or bariatric surgeon who regularly performs anti-reflux surgery and redo hiatus hernia/fundoplication work. For diagnosis and surveillance, a gastroenterologist with upper endoscopy and Barrett's expertise is usually the right door.
Use review sites as signals, then verify specialist registration, hospital profile, procedure volume and complication follow-up.
Hospital procedure explainers
These are not endorsements or a surgeon directory. They are useful hospital and academic-center pages for understanding what the operation, recovery and alternatives usually involve.
Multilingual quick guide
References and starting points